BACKGROUND:
Little is known about the risk of death among people who visit emergency departments frequently for alcohol-related reasons, including whether mortality risk increases with increasing frequency of visits. Our primary objective was to describe the sociodemographic and clinical characteristics of this high-risk population and examine their 1-year overall mortality, premature mortality and cause of death as a function of emergency department visit frequency in Ontario, Canada.
METHODS:
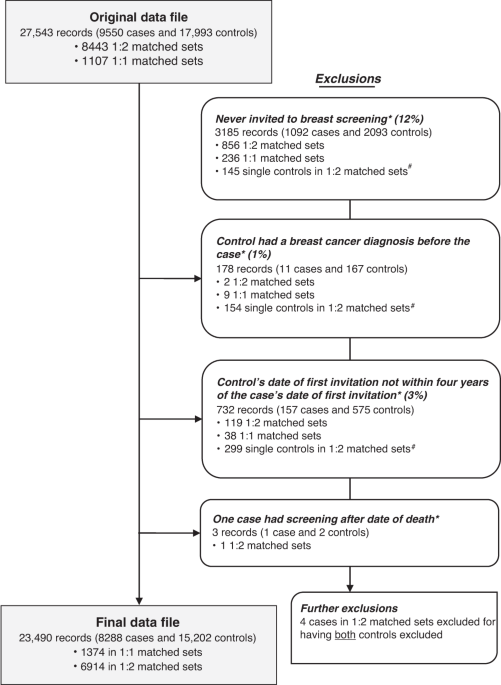
We conducted a population-based retrospective cohort study using linked health administrative data (Jan. 1, 2010, to Dec. 31, 2016) in Ontario for people aged 16–105 years who made at least 2 emergency department visits for mental or behavioural disorders due to alcohol within 1 year. We subdivided the cohort based on visit frequency (2, 3 or 4, or ≥ 5). The primary outcome was 1-year mortality, adjusted for age, sex, income, rural residence and presence of comorbidities. We examined premature mortality using years of potential life lost (YPLL).
RESULTS:
Of the 25 813 people included in the cohort, 17 020 (65.9%) had 2 emergency department visits within 1 year, 5704 (22.1%) had 3 or 4 visits, and 3089 (12.0%) had 5 or more visits. Males, people aged 45–64 years, and those living in urban centres and lower-income neighbourhoods were more likely to have 3 or 4 visits, or 5 or more visits. The all-cause 1-year mortality rate was 5.4% overall, ranging from 4.7% among patients with 2 visits to 8.8% among those with 5 or more visits. Death due to external causes (e.g., suicide, accidents) was most common. The adjusted mortality rate was 38% higher for patients with 5 or more visits than for those with 2 visits (adjusted hazard ratio 1.38, 95% confidence interval 1.19–1.59). Among 25 298 people aged 16–74 years, this represented 30 607 YPLL.
INTERPRETATION:
We observed a high mortality rate among relatively young, mostly urban, lower-income people with frequent emergency department visits for alcohol-related reasons. These visits are opportunities for intervention in a high-risk population to reduce a substantial mortality burden.